
The Condition of the United States Working Class — Where Do We Go From Here?
The Condition of the United States Working Class — Where Do We Go From Here?
In his Book, The Iron Heel, for the aliance or ‘partership’ between the labor bureaucracy and the capitalist class; As Leon Trontsky explained is his essayTrotsky and the “Iron Heel” (1937):
“One must accentuate especially the role which Jack London attributes to the labor bureaucracy and to the labor aristocracy in the further fate of mankind. Thanks to their support, the American plutocracy not only succeeds in defeating the workers’ insurrection but also in keeping its iron dictatorship during the following three centuries. We will not dispute with the poet the delay which can but seem to us too long. However, it is not a question of Jack London’s pessimism, but of his passionate effort to shake those who are lulled by routine, to force them to open their eyes and to see what is and what approaches. The artist is audaciously utilizing the methods of hyperbole. He is bringing the tendencies rooted in capitalism: of oppression, cruelty, bestiality, betrayal, to their extreme expression. He is operating with centuries in order to measure the tyrannical will of the exploiters and the treacherous rôle of the labor bureaucracy. But his most ‘romantic’ hyperboles are finally much more realistic than the bookkeeper-like calculations of the so-called ‘sober politicians.’ It is easy to imagine with what a condescending perplexity the official socialist thinking of that time met Jack London’s menacing prophecies. If one took the trouble to look over the reviews of The Iron Heel at that time in the German Neue Zeit and Vorwärts, in the Austrian Kampf and Arbeiterzeitung, as well as in the other socialist publications of Europe and America, he could easily convince himself that the thirty-year-old “romanticist” saw incomparably more clearly and farther than all the social-democratic leaders of that time taken together. But Jack London bears comparison in this domain not only with the reformists. One can say with assurance that in 1907 not one of the revolutionary Marxists, not excluding Lenin and Rosa Luxemburg, imagined so fully the ominous perspective of the alliance between finance capital and labor aristocracy. This suffices in itself to determine the specific weight of the novel.
Since One-Third of All Black Men in America Are Classified As Ex-Felons. and Black Ex-felons Have a Life Time Employment Probability Rate of 4,7%, the Actual Government Statistics Are Grossly Understated, the Overall Real Condition of the Working Class is Perpetual Pauperization!
Ten thousand times has the labor movement stumbled and bruised itself. We’ve been enjoined by the courts, assaulted by thugs, charged by the militia, traduced by the press, frowned upon in public opinion, and deceived by politicians. But notwithstanding all this and all these, labor is today the most vital and potential power this planet has ever known, and its historic mission is as certain of ultimate realization as is the setting of the sun. — Eugene V. Debs
My life has recently intersected, in a most personal way, two of Mark Twain’s famous quips. One I shall defer to the end of this essay. The other (sometimes attributed to Disraeli), identifies three species of mendacity, each worse than the one before – lies, damned lies, and statistics. — Stephen Jay Gould
I begin by stating that this essay exposes the bi-partisan lies of the capitalist class, the capitalist economists, and their media institutions, that the US capitalists has been repeating about the standard of living of the United States working class. Donald Trump’s audacity and lying are but a reflection of the level of mendacity of the United States Capitalist Class.
The last 4 decades, in the United States, have been the largest transference of wealth From the Poor, the Working class, and the Middle class, to the rich, the 1%, in the history of the world!
This has been done thorugh ‘normal exploitation’ of the working class, and through Austerity Programs (Cutting the social wages of the working class.), through Government Lies and Statistics, Usury, and with the full Compliance and Silence/Support of the United States Trade Union Bureaucracy!
In the End, we will remember not the words of our enemies, but the silence of our friends. — Martin Luther King, Jr.
Capitalism Austerity Has Meant More Wealth for the 1% and Pauperization of the 99% — Austerity means that the Rich Get Richer and the Pauperized Get Poorer
Since the 1%’s Government and their Media Monopoly has created an illusion of prosperity. And that the misleaderships of the Trade Union Bureaucracy, along with the misleaderships of the mass organizations of Blacks and other oppressed minorities, and women’s movements have supported this illusion. In the first part of this essay, I will present a series of images and quotes, to give you an idea about the real state of the United States Economy. In the second part of this essay, I will explain why the capitalists have been able to impose their worldwide austerity program and how where we should go from here.
Austerity Real State of the United States Economy
There are literally two Americas. One America is beautiful … overflowing with the milk of prosperity and the honey of opportunity. This America is the habitat of millions of people who have food and material necessities for their bodies and culture and education for their minds and freedom and human dignity for their spirits. In this America, millions of people experience every day the opportunity of having life, liberty and the pursuit of happiness in all of their dimensions. And in this America millions of young people grow up in the sunlight of opportunity. But tragically and unfortunately, there is another America. This other America has a daily ugliness about it that constantly transforms the ebullience of hope into the fatigue of despair. In this America millions of work-starved men walk the streets daily in search for jobs that do not exist. In this America millions of people find themselves living in rat-infested, vermin-filled slums. In this America, people are poor by the millions. They find themselves perishing on a lonely island of poverty in the midst of a vast ocean of material prosperity. — Martin Luther King, The Other America 4/14/1967
There are still two Americas of the those that have and those have not. Since Martin Luther King speech, there has been ‘merger mania’ resulting in an ever-increasing concentration of the wealth, in today’s world, this has division has reached such a point that now, according to Oxfam, the World’s 26 richest people own as much as poorest 50%!
While 44%of the workimg class struggles to stay alive: “Even as the U.S. economy hums along at a favorable pace, there is a vast segment of workers today earning wages low enough to leave their livelihood and families extremely vulnerable. That’s one of the main takeaways from our new analysis, in which we found that 53 million Americans between the ages of 18 to 64—accounting for 44% of all workers—qualify as “low-wage.” Their median hourly wages are $10.22, and median annual earnings are about $18,000. Brookings Institution study/”
During This Economic Crisis, Capitalism’s Three-Point Political Program has been Austerity, Scapegoat Blacks, Minorities, and ‘Illegal’ Immigrants for Unemployment, and, if opposition to austerity develops, The Iron Heel.
Democracy in the United States?: As the Capitalist Robber Barons Steal from the 99%: Only the 1% Voted For Austerity — The 99% Should Decide On Austerity — Not Just The 1% Who Profit From Austerity! Under Austerity, All of the World Will Eventually Be Pauperized, Humbled, and Desecrated Like Greece and Puerto Rico. Socialism Means True Democracy — The 99% Will Rule! — Not the Few!
In the United States, under President Obama, The Capitalist Parties (Republicans and Democrats) openly declared a policy of austerity in response to the capitalist crash in 2008-2009, as a solution to the crisis of capitalism.
Labor/Boss ‘Partnership’After I retired as a business agent for Painters Local #4 in 1997, I wrote The Fall of the Trade Union Movement in 1998. I was elected, in 1994, by the membership, who were very much aware that I was a Socialist I instantly became a part of the Trade Union Bureaucracy. Being inside the body of beast. I saw how corrupt they were. Though the Democratic Party and the Cliton Administration, they had become openly and contractorly in a Declared a Partnership with the Boss! I also learned that the Building Trades Internationals had made such a promise in 1983 and pledged to take care of any local areas, that might oppose such a partnership. (The NLRB helped them in this proces.) For a more indepth analysis of this process read The Fall of the Trade Union Movement in 1998
One result of this ‘Partnership’ Was the Complete Betrayal of the Working Class. The Betrayal has led to the unions assisting the employers to drasticly cut the standard og living of the entire Working Class!
In 2007 I updated my essay, The Fall of the Trade Union Movement in 1998, with these three paragraphs:
Leon Trotsky foretold the ‘Partnership’ Between the Trade Bureaucracy and the Boss: From Leon Trotsky and the Iron Heel:
“One must accentuate especially the role which Jack London attributes to the labor bureaucracy and to the labor aristocracy in the further fate of mankind. Thanks to their support, the American plutocracy not only succeeds in defeating the workers’ insurrection but also in keeping its iron dictatorship during the following three centuries. We will not dispute with the poet the delay which can but seem to us too long. However, it is not a question of Jack London’s pessimism, but of his passionate effort to shake those who are lulled by routine, to force them to open their eyes and to see what is and what approaches. The artist is audaciously utilizing the methods of hyperbole. He is bringing the tendencies rooted in capitalism: of oppression, cruelty, bestiality, betrayal, to their extreme expression. He is operating with centuries in order to measure the tyrannical will of the exploiters and the treacherous rôle of the labor bureaucracy. But his most “romantic” hyperboles are finally much more realistic than the bookkeeper-like calculations of the so-called “sober politicians.” It is easy to imagine with what a condescending perplexity the official socialist thinking of that time met Jack London’s menacing prophecies. If one took the trouble to look over the reviews of The Iron Heel at that time in the German Neue Zeit and Vorwärts, in the Austrian Kampf and Arbeiterzeitung, as well as in the other socialist publications of Europe and America, he could easily convince himself that the thirty-year-old “romanticist” saw incomparably more clearly and farther than all the social-democratic leaders of that time taken together. But Jack London bears comparison in this domain not only with the reformists. One can say with assurance that in 1907 not one of the revolutionary Marxists, not excluding Lenin and Rosa Luxemburg, imagined so fully the ominous perspective of the alliance between finance capital and labor aristocracy. This suffices in itself to determine the specific weight of the novel.”
When I was a painter in the late seventies, during contract negoiations, I inform my union official that we should leave wording the of the cost clause of living clause based on the 1967 COLA to remain so worded, for there was about to be a change in the official cost of living by the government. In the eighties, were got very large wage increases because the clause was never changed! We got wage increases that we never would of gotten, based on our bargaining strenth. The Fed had dropped the coat of food and gas in their new cost of living estimates The feds put ou false figures to make the economic outlook appear better than it really was.
When I started my Daily News Digest , I came across Shadow Government Statistics website written ny an honest economist — John Williams. I use mainly his charts to prove my arguments. I am an email subscriber to Shadow Government Statistis. (See his short biology, from his website below.)
* * * * * *
Walter J. “John” Williams was born in 1949. He received an A.B. in Economics, cum laude, from Dartmouth College in 1971, and was awarded a M.B.A. from Dartmouth’s Amos Tuck School of Business Administration in 1972, where he was named an Edward Tuck Scholar. During his career as a consulting economist, John has worked with individuals as well as Fortune 500 companies.Although I am known formally as Walter J. Williams, my friends call me “John.” For 30 years, I have been a private consulting economist and, out of necessity, had to become a specialist in government economic reporting.
One of my early clients was a large manufacturer of commercial airplanes, who had developed an econometric model for predicting revenue passenger miles. The level of revenue passenger miles was their primary sales forecasting tool, and the model was heavily dependent on the GNP (now GDP) as reported by the Department of Commerce. Suddenly, their model stopped working, and they asked me if I could fix it. I realized the GNP numbers were faulty, corrected them for my client (official reporting was similarly revised a couple of years later) and the model worked again, at least for a while, until GNP methodological changes eventually made the underlying data worthless.
That began a lengthy process of exploring the history and nature of economic reporting and in interviewing key people involved in the process from the early days of government reporting through the present. For a number of years I conducted surveys among business economists as to the quality of government statistics (the vast majority thought it was pretty bad), and my results led to front page stories in 1989 in the New York Times and Investors Daily (now Investors Business Daily), considerable coverage in the broadcast media and a joint meeting with representatives of all the government’s statistical agencies.
Nonetheless, the quality of government reporting has deteriorated sharply in the last couple of decades. Reporting problems have included methodological changes to economic reporting that have pushed headline economic and inflation results out of the realm of real-world or common experience.
Over the decades, well in excess of 1,000 presentations have been given on the economic outlook, or on approaches to analyzing economic data, to clients—large and small—including talks with members of the business, banking, government, press, academic, brokerage and investment communities. I also haveprovided testimony before Congress (details here).
An old friend—the late-Doug Gillespie—asked me some years back to write a series of articles on the quality of government statistics. The response to those writings (the Primer Series available at the top-center of this page) was so strong that we started ShadowStats.com (Shadow Government Statistics) in 2004. The newsletter is published as part of my economic consulting services. — John Williams
* * * * * *
Stock Market Recovery Up—No Trickle Down For The Working class!
Due the Labor Bureaucracy’s collaboration with the Boss, Real Wages Have Been Cut Over 100% Since1974! — Wages Have Not Kept Up With Inflation! Since the Neoliberal Labor Bureaucracy declared itself to be in a (Domestic) Partnership With the Boss’ (‘Bedding the Boss!’)! was fully institutionalized starting in the mid-1980s, this ‘partnership’ gave birth to the one, two, three, etc. .. wage tier system! Selling out the futures of future young workers entering the labor force. And, since the lowest union wage is immediately the highest non-union wage, this wage tier system cut the wages of the entire working class!
When I was a union official, I called this system labors’ rush to the bottom! The Graph Below is a Graphic Example of the Decline in Standard of Living of the Working Class, Since the Trade Union Bureaucracy Declared Itself to Be ‘In a (Domestic) Partnership With the Boss’(Class Cooperation)! Through the 1980s and 1990s they even included this ‘partnership’ into their work agreements and the partnership was fully established! Starting in the mid-1980s, This ‘partnership’ gave birth to the one, two, three, three, ect. wage tier system! Selling out the futures of future young workers entering the labor force. And, since the lowest union wage is immediately the highest non-union wage, this wage tier system cut the wages of the entire working class! When I was a union official, I called this system labors rush to the bottom! As in graphically shown in this: Shadow Government Statistics Graph.
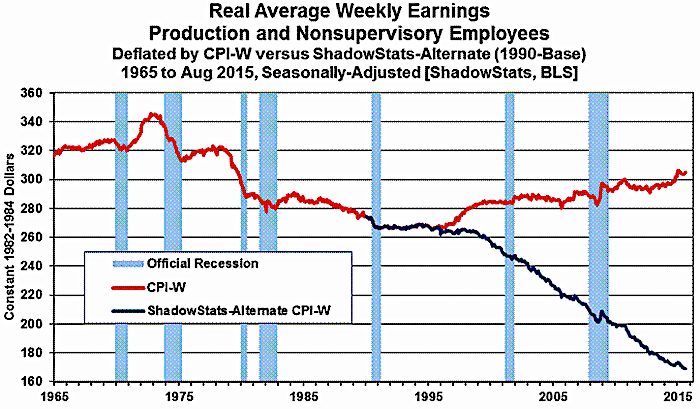
At the same time, Real Wages have Fallen Since the Wage Price Freeze of 1972 (Shadow Government Statistics): Graph 3 plots the seasonally-adjusted earnings as officially deflated by the BLS (red-line), and as adjusted for the ShadowStats-Alternate CPI Measure, 1990-Base (blue-line). When inflation-depressing methodologies of the 1990s began to kick-in, the artificially-weakened CPI-W (also used in calculating Social Security cost-of-living adjustments) helped to prop up the reported real earnings. Official real earnings today still have not recovered their inflation-adjusted levels of the early-1970s, and, at best, have been in a minimal uptrend for the last two decades (albeit spiked recently by negative headline inflation). Deflated by the ShadowStats (1990-Based) measure, real earnings have been in fairly-regular decline for the last four decades, which is much closer to common experience than the pattern suggested by the CPI-W. See the Public Commentary on Inflation Measurement for further detail. This process has led to a greater productivity and windfall profits for the capitalist, without more value being added to society.
The ‘Big Lie’ About Real Wages Has Been Going On For Decades: Shadow Grovernment Statistics Graph: Real Average Weekly Earnings- Production and Nonsupervisory Employees
Actually, the figures are even worse, if you count those who ‘don’t count’ or who were never counted, those who cannot find work and those who have been, at one time, in the prison industrial system, (See the Following Quote.)
In the last two-and-a-half decades, the prison population has undergone what the United States Bureau of Justice Statistics director Jan Chaiken last year called “literally incredible” expansion. Chaiken reported a quadrupling of the U.S. incarceration rate since 1975. That rate, more than 600 prisoners for every 100,000 people, is by far the highest in the industrialized world. The U.S. incarcerates its citizens at a rate six times higher than Canada, England, and France, seven times higher than Switzerland and Holland, and ten times Sweden and Finland. Beyond sheer magnitude, the second aspect of America’s incarceration boom is its heavily racialized nature. On any given day, Chaiken reported, 30 percent of African-American males ages 20 to 29 are ‘under correctional supervision’ — either in jail or prison or on probation or parole. Especially chilling is a statistical model used by the Bureau of Justice Statistics to determine the lifetime chances of incarceration for individuals in different racial and ethnic groups. Based on current rates, it predicts that a young Black man age 16 in 1996 faces a 29 percent chance of spending time in prison during his life. The corresponding statistic for white men in the same age group is 4 percent. According to Thomas K. Lowenstein, director of the Electronic Policy Network, 7 percent of Black children- nearly 9 times more than white children- have an incarcerated parent. — Race, Prison, and Poverty
July 24,2020 Update: Since One-Third of All Black Men in America Are Classified As Ex-Felons. amd Black Ex-felons Have a Life Time Probability Rate of 4,7%, the Actual Government Statistics Are Gossly Undersated, the Overall Real Condition of the Working Class is the Process of Pauperization!
The following quote and graphs from the Brookings Institution article, Brookings: Meet the LOW-Wage Workforce are a graphic example of the pauperization of the Working Class.: “Describing Low-Wage Workers More Than 53 million people—44% of all workers aged 18-64—are low-wage workers by our criteria. They earn median hourly wages of $10.22 and median annual earnings of $17,950.”
Pension Robbery Swindle
Pensions of Union Workers Cut in Federal Budget (Video Interview with Michael):
DESVARIEUX: So, Michael, today we’re going to be talking about the federal budget. What has really stood out to you in that budget?
HUDSON: Well, there’s something very radical happened, that people haven’t been talking about very much. Normally a budget is supposed to decide what gets funded and what doesn’t get funded, and it’s simply a decision of what to cut back. A budget is not supposed to rewrite the law. But what happened is something very radical. They rewrote two laws. One of the laws was about bank derivatives that Elizabeth Warren has spoken about, promising to bail out Citibank and other banks. If they lose on derivatives, they’re going to get bailed out like they did in 2008.
And the other was a decision not to bail out the Pension Benefit Guaranty Corporation, the government’s pension fund insurer. They’ve decided–they passed a new law. They rewrote the law. They declared the 1974 ERISA act protecting pensions illegal, and they said if pension funds cannot pay their retirees, they get to be cut back and they don’t get to go to the government to get a guarantee. We’ve abolished the government guarantee on pension funds if the pension fund is run by a labor union, meaning if a pension fund is a multiemployer fund that has more than one employer contributing to it, like airline funds, truckers funds, Teamsters funds if you’re a truck driver, insurance employees, we’re going to give the fund managers, mainly the financial managers on Wall Street, the right to cut back on these pensions that are due. So the pensions that people had expected to receive when they made their wage contract saying, well, we’re not going to ask for as fast a wage increase if you give us security when we retire, all of this has been rewritten.
And the ironic thing is the Democrats led this fight against labor a year ago, this special ruling was put in, and people who were supposed to be Democratic liberals, like Marcy Kaptur of Ohio, decided to have something also radical in the new budget. They weren’t going to report which representatives voted yes or no for these amendments. So the Democrats covered up their tracks, and you can’t see that they were really behind the Wall Street constituency in saying, we’re going to cut back the pensions. And you can see what’s on the mind, basically. The government said, look, we’ve got to balance the budget in the face of Obama’s sort of escalating the military confrontation with Russia and China. And on the face of an increased bailout for the banks, there’s just not going to be enough money to guarantee the pension funds. So we can’t do for the pensioners what we did for the bankers in 2008.
So this has turned out to be just an absolute disaster. Yeah, it looks like a lot of union pension funds and public service pension funds are going to go the way of what happened in Detroit and California cities, of being cut back when there’s not enough. And part of the problem is that these pension funds were all set up in a way that they were guaranteed to lose. The whole idea was to pretend that companies didn’t have to pay very much to support their workers or to put money aside to pay pensions, because they said, look, these funds can make money on Wall Street, they can make eight and a half percent a year. Well, as it turns out, pension funds are not making eight and a half percent a year; they’re making–if they want to be safe, they’re making less than one percent a year, which is the government Treasury bill rate.
So what they’ve done is they’ve gotten sort of desperate, and a lot of pension funds have gone to pension to hedge funds and Wall Street. They’ve gone to Wall Street money managers and said, look, can you–we’re desperate, we’re going to have to go under; can you help us make more money? Well, the Wall Street sharpies think, well, okay, sure, we’re going to put your money in derivatives and other things. And the banks that have been managing these funds, like Goldman Sachs and Northern Trust, have actually done very badly. And the most troubled fund of all of the ones in question are the Teamsters fund for the central states of America. And the government’s trying to blame labor very much in the way that Malthus blamed labor a few hundred years ago for its poverty. The whole idea is, well, a few years ago there were, like, four workers for every retiree, so it was easy for the workers to pay into the funds and organize it sort of like a Ponzi scheme, keep paying in, and there was enough to pay. But now that the economy’s been de-industrialized, there are more retirees for every worker. So the Obama administration is saying, well, the problem is that there are just not enough workers to pay. Sorry, they lose.
But the Congressional Budget Office has found that that’s really not much of the problem at all. A lot of the problem is that the pension funds have gotten desperate, turned over their money to Wall Street. Some of this was done under the Congressional and Justice Department force. A lot of union pension funds, especially the Teamsters, were run by the mafia. So the government said, well, look, the mafia are crooks; let’s turn the money over to Wall Street. What they didn’t realize is that Wall Street people are just as crooked as the mafia, and they did pretty much a strategy that was pioneered, I think, by Prudential Insurance a couple of decades ago, back a generation ago. Every day, Prudential would buy and sell a given stock. If the stock went up, they’d put the gains in their own account; if the stock went down, they’d say, oh, that’s the accounts of the clients we’re managing. Well, that’s pretty much what Wall Street’s been doing with the pension funds. They’ll play both sides of the derivative gains. They keep the gains for themselves and pay themselves bonuses and high salaries, and the losses are all stuck to Orange County or Detroit or Birmingham, Alabama, or other public funds. And there have been a number of lawsuits where Wall Street’s had to give back the money. And they’ve all been accused of fraud.
But the Justice Department said, well, wait a minute. These banks who were cheating the pension funds are too big to fail. They’re systemic. We can’t throw Citibank in jail. We can’t go against Northern Trust. So, essentially, now that Wall Street has realized that there is nothing to stop them from ripping off the pension funds, this is the largest single volume of capital to be grabbed. And that’s up for grabs. And, basically, this is the first step towards the fight they’re going to be seeing over the next two years to balance the budget by cutting back Social Security, which has been Obama’s chief economic aim from the beginning, and then to privatize pensions and to privatize Social Security. The argument’s going to be made to American workers, well, wait a minute, you’ve seen your pension funds aren’t able to pay, you’ve see them lose money on derivatives. There’s only one way to be safe: take responsibility for yourself, and you manage your own money in the 401(k)s and the other personal programs.
So they’re going to privatize all of the pension funds. And by making your own choice, what this really means is the individual employees are going to have to turn over their funds to the same Wall Street companies–Goldman Sachs and Northern Trust–that have managed the–mismanaged the corporate pension funds and the union pension funds. And so the whole idea is that all of a sudden, now that employment is not growing, now that wages are not growing, instead of making profits by underpaying labor, Wall Street’s going to make profits just by siphoning off all of the savings that have been put aside in advance to pay the pensions. The argument will be, I’m sorry, folks, there’s not enough to pay the pensions or the Wall Street calculators who made these forecasts made a terrible mistake. Unfortunately for you, under the law that Congress has just rewritten, not only do they get paid before you, but we’ve just canceled the government’s responsibility to insure you. We’ve taken away your insurance. That’s going to be the fight that we’re seeing. And now that the Republicans are in control of both the House and the Senate, the Democrats can say, ah, let’s support Wall Street and blame it all on the Republicans. And they’re going whole hog, really, to stiff the pension retirees.
Federal Government Keeps Cheating Retired Seniors— The Federal Government’s ever-changing cost of living index.: Retired workers living on social security, are cheated out of social security wage increases by 5%, if you used how the government ‘figured’ the social security increased in 1990, and by 8% how it was ‘figured’ in 1980. Our ‘labor leaders have remained silent in their duty to their partners. The graphs below demonstrate the 1% government’s sleight of hand.
Shadow Government Statistics Alternate Inflation Charts Alternate Inflation Charts The CPI chart on the home page reflects our estimate of inflation for today as if it were calculated the same way it was in 1990. The CPI on the Alternate-DataSeries tab here reflects the CPI as if it were calculated using the methodologies in place in 1980. In general terms, methodological shifts in government reporting have depressed reported inflation, moving the concept of the CPI away from being a measure of the cost of living needed to maintain a constant standard of living.
Since June 2009 Americans have lived in the false reality of a recovering economy. Various fake news and manipulated statistics have been used to create this false impression. However, indicators that really count have not supported the false picture and were ignored. For example, it is normal in a recovering or expanding economy for the labor force participation rate to rise as people enter the workforce to take advantage of the job opportunities. During the decade of the long recovery, from June 2009 through May 2019, the labor force participation rate consistently fell from 65.7 to 62.8 percent. —Paul Craig Roberts, The Diminishing American Economy
Bureau of Labor Civilian Labor Force Participation Rate is 63.9%
The Above Graph and Quote Proves the Accuracy of Shadow Government Statistics Alternate Unemployment Charts. The seasonally-adjusted SGS Alternate Unemployment Rate reflects current unemployment reporting methodology adjusted for SGS-estimated long-term discouraged workers, who were defined out of official existence in 1994. That estimate is added to the BLS estimate of U-6 unemployment, which includes short-term discouraged workers. The U-3 unemployment rate is the monthly headline number. The U-6 unemployment rate is the Bureau of Labor Statistics’ (BLS) broadest unemployment measure, including short-term discouraged and other marginally-attached workers as well as those forced to work part-time because they cannot find full-time employment.
Another aspect is that the real unemployment rate is at 1930s depression levels.: Shadow Government Statistics Alternate Unemployment Charts The seasonally-adjusted SGS Alternate Unemployment Rate reflects current unemployment reporting methodology adjusted for SGS-estimated long-term discouraged workers, who were defined out of official existence in 1994. That estimate is added to the BLS estimate of U-6 unemployment, which includes short-term discouraged workers. The U-3 unemployment rate is the monthly headline number. The U-6 unemployment rate is the Bureau of Labor Statistics’ (BLS) broadest unemployment measure, including short-term discouraged and other marginally-attached workers as well as those forced to work part-time because they cannot find full-time employment.
U.6 and Shadow Government Statistics Alternate U.S. Unemployment Rates Headline (U.3 and U.6) versus ShadowStats Alternate 1994 to November 2019, Seasonally-Adjusted [ShadowStats, Bureau of Labor Statistics]Robber Baron Usury Capitalism in the United States
A new factor has been added to the exploitation of the working class and oppresion of the mases — Robber Baron—Style Uaury!
The 1%’s Billion Dollar GovernmentUsuury: the practice of making unethical or immoral monetary loans that unfairly enrich the lender. Originally, usury meant interest of any kind. A loan may be considered usurious because of excessive or abusive interest rates or other factors. Historically, in some Christian societies, and in many Islamic societies even today, charging any interest at all would be considered usury. Someone who practices usury can be called a usurer, but a more common term in contemporary English is loan shark.
Robber baron, pejorative term for one of the powerful 19th-century U.S. industrialists and financiers who made fortunes by monopolizing huge industries through the formation of trusts, engaging in unethical business practices, exploiting workers, and paying little heed to their customers or competition. Alternatively, those who credit the explosive growth of American capitalism during this period to the indefatigable pursuit of success and material wealth are likely to celebrate these entrepreneurial tycoons as “captains of industry.” Among the sectors in which they compiled their great wealth were the oil, steel, liquor, cotton, textile, and tobacco industries, railroads, and banks.
It took 100 years, but America has returned to its unequal past. With a vengeance. — America 2018: Even More Gilded Than America 1918
- Related Article: “A Ponzi Scheme” The Economy is Only A Paper Moon
2019 Update: The Banks are Now Making a Profit Risk Free:
When Mary Poppins was made into a movie in 1964, Mr. Banks’ advice to his son was sound. Banks were then paying more than 5% interest on deposits, enough to double young Michael’s investment every 14 years. Now, however, the average savings account pays only 0.10% annually – that’s 1/10th of 1% – and many of the country’s biggest banks pay less than that. If you were to put $5,000 in a regular Bank of America savings account (paying 0.01%) today, in a year you would have collected only 50 cents in interest. That’s true for most of us, but banks themselves are earning 2.4% on their deposits at the Federal Reserve. These deposits, called “excess reserves,” include the reserves the banks got from our deposits, on which they are paying almost nothing; and unlike with our deposits, there is no $250,000 cap on the sums banks can stash at the Fed amassing interest. A whopping $1.5 trillion in reserves are now sitting in Fed reserve accounts. The Fed rebates its profits to the government after deducting its costs, and interest paid to banks is one of those costs. That means we the taxpayers are paying $36 billion annually to private banks for the privilege of parking their excess reserves at one of the most secure banks in the world – parking their reserves rather than lending them out. The banks are getting these outsized returns while taking absolutely no risk, since the Fed as “lender of last resort” cannot go bankrupt. — Ellen Brown, Why Is the Fed Paying So Much Interest to Banks?
The Vertual Elimination of Usury Laws in the United States
In the 1960s, when credit cards were being established by the Banks, a series of State Government and Supreme court decision made usury legal. State Usury laws were thrown out by the Supreme Court if the Banks moved their headquarters into states that not have strict or any usury laws. Thus credit cards charged 17% ‘loan shark loans’ if credit card loans were not paid in full.
As a result, the working class was buying cars, other commodities,ect., with credit card debt. Not to be outdone by the banks, the Federal Government made ‘loans’ to poor, working-class, and middle-class college students, in order to get a college education. The real education has been that in today’s world, these loans will never be paid off and neither will the growing interest debt. The majority of the populaion will never get out of debt. The below graphs show the extent of the ever-growing debt.:
Average Credit Card Debt in America: September 2019
Why Does The US Gov’t Charge Interest On Student Loans? Why Is The US Gov’t Effectively Engaging In Usury With Such A Fundamental, Public Good?(Note That Usury Spiked After the 2008 Crash)
None of the above changes in the United States, by the Capitalist Class,could have been made, if not for the betrayal, collaboration, support, default, and/or silence of the United States Labor Bureaucracy. That became codified in the 1980s through the slow application of the Taft Hartley and Kennend, Landrum, Griffin laws.
The Way out of the Current Condition.
All is not lost, for today’s youth, due to these austerity laws, that they inherited from their forefathers. Are opposed to the austerity political programs of the world capitalist class.
The majority of today’s are sympathetic to socialism! This is shown by the support for Social Democrats like Bernie Sanders. However, the Social Democrats do not and have not directly opposed Capitalist Austerity.
As the Capitalist Thieves Steal from the 99% — Only the 1% Voted For Austerity — The 99% Should Decide On Austerity — Not Just The 1% Who Profit From Austerity! Let the 99% Vote on Austerity!
Austerity is a Political Progam, and it Must be Oppose Politically.
In most of the countries in the world, there are working-class and Socialist Parties. Through the default of the Trade Union Bureaucracy and their political party, the party of Obama austerity, the working class has no voice for their frustration with austerity.
I believe, at his time, that, at his time, it is utopian to call for a labor party, based upon the trade union bureaucracy. But rather, socialist should speak out against austerity and try to form an anti-austerity organization, study groups, clubs, ect., to begin a discussion of how to fight back under the present conditions. We must educate, agitate, and organize against austerity.
Just as I wrote these words, it seems that the Rank and File Workers want a change. Today’s (September 16, 2019) headlines:
46,000 UAW Workers Strike at GM Plants NationwideCanadian Aluminum Workers Launch Factory OccupationIn a rare move, hundreds of workers of the Nemak aluminum factory in Windsor, Canada, decided to occupy their factory when it was announced that it would close down soon. Pablo Vivanco reports
‘When We Fight, We Win’: Protesting Stagnant Wages as GM Rakes in Record Profits, 50,000 Auto Workers Go On Strike“We are standing together in unity and solidarity for our members, their families, and the communities where we work and live.” Demanding fair wages, decent healthcare benefits, and their share of General Motors’ “record-level profits,” nearly 50,000 United Auto members went on strike just before midnight Sunday following failed contract negotiations. “Today, we stand strong and say with one voice, we are standing up for our members and for the fundamental rights of working-class people in this nation,” said UAW vice president Terry Dittes ahead of the strike, which will grind to a halt dozens of plants across the U.S. By Jake Johnson“The Rank and File Have to Take Control!”: Ford, Fiat-Chrysler Workers Call for All-Out Strike Alongside GM WorkersAt midnight Sunday, roughly 49,000 autoworkers struck at General Motors (GM), shutting down production at the largest US-based automaker. The strike is a major episode in the resurgence of the class struggle. American autoworkers are now at the tip of the spear of a global counteroffensive by workers against poverty, inequality and job losses, encompassing not only autoworkers but teachers, public transit workers, Amazon workers and the entire working class. Overnight, things rapidly happen. This response tby UAW workers in Canada and the United States, hopefully could be a sign of a beginning of a fight against the austerity policies of the last four decades. These strikes deserve our full support! A working-class victory could be a beginning of the rise of the calss struggle. We must oppose an expose any government and labor bureaucracy intervention to organize a defeat!
Based upon past history a rapid rise in the militancy of the United States Working Class has happened after a long endurance of of Capitalist Classes’s attacks against the lowering of labor’s standard of living. Also, based upon past history, the United States Working Class has moved in an apolitical direction. – the Rise of the Socialist Party and E.V. Debs after the last Guilded Age in the United States (1870-1890(.
There is also a bright light in the world picture. Jeremy Corbyn an anti-war leader and Labour MP, who, in 2017, got elected as the leader of the British Labour Party, running against the Labour Party Blair Leadership, who had complied with the austerity program imposed upon the working class by the 1% in the United Kingdom. This was and entrenched Bureaucracy like the U.S. Trade Union Bureaucracy
Corbyn ran on a clear program against austerity. He spoke at mass rallies of workers he agitated against austerity. And hundreds of thousands of young workers joined the Labour Party to elect Corbyn!
Jeremy Corbyn Speaking at a 2017 Campaign Rally
The specter of Jeremy Corbyn has terrorised the Capitalists!
Video: Jeremy Corbyn tells Morgan Stanley: ‘You’re right, we are a threat’ Jeremy Corbyn has told Morgan Stanley it is right to regard him as a threat, after the investment bank warned its clients that a Labour government could pose as much of a risk to British business as Brexit. The Labour leader hit back on Thursday, accusing Morgan Stanley of being part of the same “speculators and gamblers who crashed our economy in 2008”. In a video posted on social media, he also promised a new approach to financial services regulation. “Nurses, teachers, shopworkers, builders, just about everyone is finding it harder to get by, while Morgan Stanley’s CEO paid himself £21.5m last year and UK banks paid out £15bn in bonuses,” Corbyn said.
“Labour is a growing movement of well over half a million members and a government-in-waiting that will work for the many. So when they say we’re a threat, they’re right. We’re a threat to a damaging and failed system that’s rigged for the few.”Corbyn said the greed of bankers had plunged the world into crisis a decade ago and the UK was still paying the price because the Conservative party had “used the aftermath of the financial crisis to push through unnecessary and deeply damaging austerity”. “That’s meant a crisis in our public services, falling wages and the longest decline in living standards for over 60 years,” he said. He highlighted Morgan Stanley’s $3.2bn settlement with US authorities for its role in the creation of flawed mortgage-backed bonds during the global financial crisis, and the bank’s four meetings with senior government figures including Philip Hammond, the chancellor, last year. Corbyn said Labour would soon be publishing policies on the finance sector and how it planned to transform the economy. He was moved to record the video, posted on his Twitter feed and Facebook page, after Morgan Stanley released a note telling investors about what it perceived as the risks of Corbyn taking power.
Morgan Stanley warned about the nationalisation of key industries, higher taxes and a shift in spending priorities towards low-income households under Corbyn’s leadership, which it said could damage valuations of UK companies.
It told investors that another general election was likely towards the end of 2018 once Theresa May’s government realized it could not secure the Brexit deal it wants and the Tories began to fall apart, opening the door to Labour taking power.
“The UK is in the midst of a double whammy of uncertainty in the shape of Brexit and a fragile domestic political situation. Taken together, these two factors – which are interrelated to some degree – cast a long shadow over the policy backdrop and economic outlook of the UK,” the report from Morgan Stanley’s European equity team said.
“For the UK market, domestic politics may be perceived as a bigger risk than Brexit. From a UK investor perspective, we believe that the domestic political situation is at least as significant as Brexit, given the fragile state of the current government and the perceived risks of an incoming Labour administration that could potentially embark on a radical change in policy direction.
“Against this backdrop, even if we see good progress in the Brexit negotiations, the scope for UK sensitive assets to rally may be muted unless we also see an improvement in the government’s position in opinion polls.”
Morgan Stanley said British utility companies, especially in the water and power sectors, were most at risk from a Labour government, but postal services, telecommunications and travel companies could also be affected.
Higher taxes and a corporation tax rise to 26% might damage British financial services, Morgan Stanley said.
“Spending priorities … shift in favor of low-income households and the public sector and away from outsourcers and defense companies,” the report continued. “Higher low-end wage growth could also impact service-oriented companies with low margins, such as retailers.”
From Britain: Victory for Corbyn! The genie is now out of the bottle:
As the Financial Times, gritting its teeth, commented: “Jeremy Corbyn has returned as leader of Labour, tightening the grip of the hard leftover one of Britain’s oldest political parties.” The ruling class is alarmed at this advance of the left and will do whatever they can to stop it. The right-wing is a Fifth Column of big business within Labour. They are careerists like their counterparts in the capitalist parties. They will jump ship when the time comes. Britain is heading into unchartered waters. The Tories, although repackaged, are heading for a bust-up over the Brexit negotiations. The splits in the Tory Cabinet can already be seen. This is simply a foretaste. With a new economic crisis, the scene will be set for a general election showdown. At that point, the capitalist Establishment may call on the right-wing in the Labour Party to split to prevent Corbyn coming to power.
Jeremy Corbyn at the National Anti-Austerity March 20/06/2015After the election. the labour party put forth a Manifesto against austerity, under the slogan; For the Many — Not the Few! For the 99% to decide their own fate For the Many Not the Few!
{kind=link}
Using the Monarchy, the British Capitalist Class has undermined parliamentary in England, suspended parliament, and called for elections.
The response of the young working class has been for over 200 hundred thousand young workers to join the Labour Party to fight against Austerity and the threat to democracy! A victory for Labour could become a poll for the workers of the world.
To end austerity, intimately, we must work to build one, two, three, and many working-class political parties. And develop a new world working-class order, under the slogan, For the Many Not the Few! With this goal we can begin to build a more effective worldwide movement. Against the Capitalist Robber Barons who steal and have stolen the world’s wealth from the 99%! Fight Against Austerity!
As the Capitalist Thieves Steal from the 99% — Only the 1% Voted For Austerity — The 99% Should Decide On Austerity — Not Just The 1% Who Profit From Austerity! Let the 99% Vote on Austerity!
Obamas’ and the 1%’s Political Program, After the 2008 Crash has Been to Bailout and Protect Capitalism the 1% and to Attack the Standard of Living of the 99%. Must Oppose Austerity In the United States and World-Wide! — To Begin, We Should Form a National Coalitions of Workers, Blacks, and Oppressed Minority Coalition to Call For a National March Against War, Poverty, and Austerity In Washington DC!
Posts navigation
← Contradictions of the UAW GM Strike
“Trade Secrets” Cancer and the Environment (What the Bill Moyers Program “Trade Secrets” Revealed) →